Few things have riled up the Glibertariat lately as much as the title of Dr. for PhDs and Doctorates. It’s currently 4:30am but DST (another hot topic) tricked me into thinking it’s 5:30am. The idea of this article started running through my head so, what the hell, let’s give it a try.
I’m going to take the unpopular position here that PhDs have just as much a right to the Dr. title as physicians. For full disclosure, I am working towards my PhD now, but this has been my inclination since well before going back to school.
I am not a linguist, so HM feel free to jump in here about how wrong I am, but I believe Dr. was originally reserved for teachers. Not the half-educated babysitters we largely have now in the teaching profession, but rather actual learned men who would be the precursor to the PhD. It wasn’t until much later did physicians also receive the title of doctor. According to Merriam-Webster:

Richard Rolle, 14th century theologian and mystic
The English language history of doctor starts in the early 14th century, when the word was first applied to a select few who likely knew neither bloodwork nor basketwork. They were equipped for dealing with matters of the soul: they were eminent theologians who had a special seal of approval from the Roman Catholic Church as people able to talk about and explain the doctrines of the Church. They were teachers of a kind, and the word’s origin makes this connection. The word doctor comes from the Latin word for “teacher,” itself from docēre, meaning “to teach”.
So we’ve established that PhDs were using the title well before physicians. If there’s going to be a dispute about this, then MDs should really go by Physician X, not Dr. X. Still, there’s been a lot of chatter about physicians having a right to the title and not PhDs. This hasn’t been my experience at all coming from physicians or shot callers in the health industry. When you’re giving a presentation to a group of physicians, hospital administrators, or regulators on an innovation, they want the presenter to be announced as Dr. X, PhD or MD. As it’s been explained to me by the pros who wine and dine these groups for a living, all they really care about is that the presenter can be called Dr. So and So. Which is why I don’t understand the “Is there a doctor in the house argument?”. This is a colloquial phrase, and really should be asked is if there is a physician in the house. Which is kind of stupid because, again, MD is a highly specialized and technical skillset. Unless if the MD is trained in the ER specialty, they are going to bring the same kind of skills that a paramedic or nurse would. In fact, if I’m having a health emergency in public, I’d much rather a paramedic step forward to help than a psychiatrist or an ophthalmologist. Let’s put this “doctor in the house” saying to bed.
The next argument I’ve been reading is that MDs go through rigorous training that has a narrow cutoff that makes them somehow above us other mortals and uniquely qualified for the title of “Dr”. That may have been true once upon a time, but just isn’t the case anymore. Medical school admittance is tightly controlled by the AAMC guild. Capacity has not kept up with the demand, and it is now at the point where they have easily double the number of qualified applicants versus open spots. This means the best and brightest no longer need to be selected for medical school but rather so many candidates meet the technical bar that other attributes can be selected for. I don’t remember the exact saying we use here on the Glibs, but the whole progressives infiltrate a respected institution, gut it, and wear it as a skinsuit applies to medical schools. The MCAT, the medical school admissions test, now screens for social justice warrior attributes through a recently added test section. From the Washington Examiner:
But it is Kirch’s reform of the MCAT that raises the most concern. The AAMC began redesigning the test in 2009, but only received approval for the revisions in 2012. In an announcement reported by the New York Times that year, Kirch explained, “The goal is to improve the medical admissions process to find the people who you and I would want as our doctors. Being a good doctor isn’t just about understanding science, it’s about understanding people.” One new section of the exam, entitled “Psychological, Social, and Biological Foundations of Behavior,” requires test-takers to respond to multiple-choice questions in which both the question’s premise and the available answers are, at best, often distantly related to medicine.
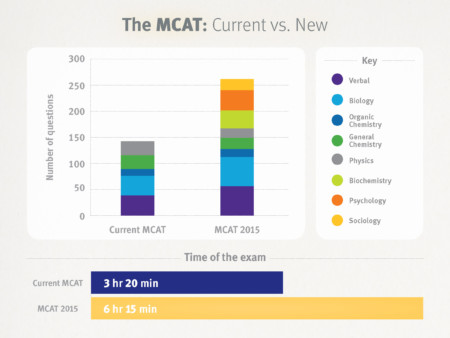
“New” is the MCAT 2015 version
One MCAT practice question (from a collaboration between the AAMC and online-education nonprofit Khan Academy), for example, asks whether the wage gap between men and women is the result of bigotry, sexism, racism, or biological differences (no other options are provided, and the “correct” answer is sexism). Another asks whether the “lack of minorities such as African Americans or Latinos/Latinas among university faculty members” is due to symbolic racism, institutional racism, hidden racism, or personal bias (the correct answer is institutional racism). Yet another asks test-takers to select from a list of debatable definitions for “the terms ‘sex’ and ‘gender.’ “
Here’s a quote on the AAMC’s website from an accepted student that illustrates what their “right fit” student is:
“I personally see medicine as a component of social progress and justice. Loyola Stritch School of Medicine is immensely dedicated to social justice and involvement with marginalized and vulnerable populations, therefore it was a great fit for me.”
-Moron, accepted student to Loyola Stritch School of Medicine

And of course, lest you think that this just applies to entry classes and not the curriculum, Medical Schools are adjusting their curriculum to incorporate less medical knowledge in favor of adding social justice components. Here’s a blurb about the newly redesigned curriculum at Yale, School of Medicine:
Although that night’s class imparted a specific lesson, it was part of an 11-session course with a larger purpose. Its goal was to teach students in the health professions how to speak to people who come from different backgrounds and life experiences and help students develop the skills to serve as advocates for vulnerable populations. Two second-year med students, Tehreem Rehman and Robert Rock, saw a need for this type of training in the medical school curriculum, as well as more discussion of health equity. “We only had one or two sessions on health disparities,” Rehman said. “We felt a dearth of that.” With support from faculty, they designed U.S. Health Justice and offered it for the first time last fall. Their model was a global health program that had also been initiated by students and ultimately became a course of study that now offers the Certificate in Global Medicine. “We didn’t want this to be a one-time class,” said Rehman. “We really were hoping this would start momentum and get health equity in our education.”
The students’ proposal came as the medical school is launching a revised curriculum, and a key element is medicine’s responsibility to society. “We were aware of the school’s ongoing initiatives to reform the curriculum and sought to use that to our advantage,” Rehman said.
So can we put this notion to rest that today’s physicians are gods above men that somehow uniquely deserve the title of “Dr.”? The next argument I’ve heard is that PhD should only use their title on the conference circuit or while teaching and not elsewhere. I don’t really understand this. A title is a title. No, you shouldn’t introduce yourselves to your neighbors as Dr. X when you have a PhD. But you shouldn’t do this with an MD either. I think it’s obnoxious to use a title at all in friendly social contexts. There was a lot of sneering at Christine Ford for being referred to as Dr. Ford. Frankly though, there’s no way in hell I wouldn’t put Dr. SSD for anything involving my interaction with the government. The government and private institutions thrive on credentialism these days and, right or wrong, you’re intentionally shooting yourself in the foot if not listing your credentials. You can bet when I’m going up against the assholes on the local school board or zoning committee that I’ll be using Dr. SSD and not Mr.

Finally, the last argument is that if PhD can use the title “Dr.”, what about those with doctorates? I don’t know, the rapid growth of doctorates is a recent phenomenon and goes hand in hand with the above credentialism point. PhD programs are much more rigorous than a doctorate and involve original research components. In Europe, doctorates are viewed more as a technical degree. Here in America, many programs that were formerly master’s level are now calling themselves doctorates without any real difference. For example, new physical therapists are now required to obtain a doctorate in physical therapy to practice. However, the doctorate program just replaced the former master’s program without any progression. This move to doctorates is coming for the other types of therapists too. And yes, I have seen a physical therapist introduce themselves in social situations as Dr. X because of that doctorate. It’s bizarre, but again, still obnoxious for anyone to introduce themselves as Dr. X in social situations. There are older professions, such as lawyers, with a more rigorous and traditional doctorate. Should lawyers be titled with Doctor? I think they have more of a right to it than the PTs. Lawyers used to have esquire after their name, and this is still frequently used in the South. Perhaps lawyers should have their own title… it would certainly help to identify them as a warning to others.
Just kidding to our resident Glib lawyers… well kind of.
SSD Note: this article is partly tongue-in-cheek ….no offense intended to our resident Glib physicians… unless if you answered the above practice MCAT questions correctly.
Call me Doctor Proctor
Call me Dr. Love [waggles eyebrows]
Yes, Mr. Simmons.
Dr. Johnny Fever
Dr. Feelgood?
Dr. Trump
Col. Doctor
Dr. Detroit!
Based on the corners in which I’m expert, I’m shocked half of us aren’t killed every day.
Doctors are men who prescribe medicines of which they know little, to cure diseases of which they know less in human beings of whom they know nothing – Voltaire
“I’m shocked half of us aren’t killed every day.”
Me too.
A hottie in a brand new mustang passed me in a curve the day before yesterday. She had to be going 80mph. Two miles down the road she pulled into a store parking lot.
Oh, sorry about that.
Heh. This made me laugh.
:BRAVO:
If you pass on the left and your pull-off didn’t cause me to touch my brakes, no foul is recorded.
Same here. I swear, USians don’t know what the left lane is for.
My lead-footed mother calls them “speed monitors.” I wouldn’t go so far as to say they’re trying to police others’ speed, but I am convinced they’re just not paying attention and they don’t seem to know what flashing lights behind them means.
And tailgating does not work. They are NOT PAYING ATTENTION.
To be fair, almost all of the assholes I’ve encountered flashing their lights and tailgating (and honking) are too impatient to let me pass the truck on my right. Granted, I don’t linger in the left hand lane if I don’t have to.
My rule of thumb is if there’s a slow poke in the left hand lane, I pass on the right. If I can’t pass on the right, then they’re using the left hand lane correctly, and I’m the dillhole for being impatient.
If some hothead starts tailgating, honking, and/or flashing their lights at me while I’m in the left hand lane, they’re liable to get brake checked or I’ll just let off the gas and coast down until I can merge back to the right.
This, they’ll tell you they’re mad because you’re ‘hanging out’ in the left lane not that you aren’t passing people fast enough. If you are ‘Hanging out’ in the left lane and they are driving like they claim everyone should then you wont be in their way anyhow.
Oh, if someone is in the left lane going faster than the dude in the right lane with the clear intention to pass, but they are still going slower than I am, I’ll be impatient, but understand that they are going to pass but would prefer not to do it as quickly as I would.
The only thing that will get me is when someone won’t speed to pass. I’ve seen this on the two lane highways with out-of-staters who clearly want to pass the person because they are going 79, but the passer is only willing to go 82 to pass. Freaking speed up, get around and then drop speed to the speed limit if you need to but don’t inch forward going 1mph faster than the guy you are trying to pass.
If we want to talk about asshole driving, what about those dick heads who accelerate when you try to pass them. I’m going 2-4 mph faster than them with cruise on, pull out to pass, get abreast of them, and all of a sudden I’m going 5 mph slower than them. That gets me ragey really fast.
You need a faster car, trashy.
Again I’m with SO. Trshmnstr esq., I get not everyone likes using cruise control (they’re wrong but I get it) But even if you don’t like using cruise control it shouldn’t be that hard to maintain a fairly consistent speed on the open road.
That makes me see red.
What was always funny, though, was when it was some punk in a newer car than my old Granny (96 Olds with nonexistent clear-coat), thought they could out-run me.
Yeah, no, kid. This car takes mountain passes like they’re straightaways.
Indeed they are wrong, but I do NOT get it.
Also. I do drive too fast. That is true. I shouldn’t.
I just have this thing where I want to get where I am going as quickly as possible. I don’t speed for any thrill or any intention of showing off or whatever. I just want to Get There. It’s also why I never stop at roadside touristy things when I’m roadtripping.
I’m a +7 driver. I get to speed limit +7, set the cruise, and done. Obviously I adjust if the prevailing speed is very different, but I’m torn between wanting to get there fast, and not wanting a ticket.
USians don’t know what the left lane is for
It is for hauling your giant boat to the cabin with your underpowered mini-van. So you don’t have to hassle with people trying to merge onto the highway in the right lane.
What do I win?
No, the left lane is so that traffic only appears on your right, giving you time to browse Facebook, Twitter, and Instagram. When your exit finally comes up, erratically veer across three lanes.
That’s it. I expect you pukes to address me as Captain Spud from now on.
Sorry, Licious.
That is COLONEL Swiss to you!
/Senator Ma’am
Looks at USAA mail
“Yes Sir, Sir”
That sounds like a good name for a sandwich.
“Excuse me, could I have a Colonel Swiss with fries?”
I have no dog in this fight except a strong linguistic opinion: That of “shorthand.”
We have linguistic shorthand that is a cultural norm. Even though it’s sometimes imprecise, it gets the point across to native English speakers.
Whether it’s “proper” or not is totally irrelevant. A random person says “doctor,” they mean MEDICAL DOCTOR. It is understood. The fact that you have to CLARIFY that you are not a MEDICAL DOCTOR buttresses my assertion.
The problem is really douchebags who refuse to observe the cultural/linguistic shorthand.
=========
After having worked in the field of medical malpractice litigation on the plaintiff’s side, I have the longstanding opinion that lawyers are smarter than doctors and that doctors are mechanics. Some of them are better mechanics than others. And the bad mechanics need to be sued right out of existence.
The problem is really douchebags who refuse to observe the cultural/linguistic shorthand in a moment when it is clear that a MEDICAL doctor is needed.
“Is there a doctor in the house?” is not the moment someone other than a MEDICAL doctor needs to raise their hand.
This gets said brought up a lot. I doubt it has ever actually happened.
I’m going to leave the lawyers are smarter than doctors comment alone because lawyers are not supposed to damage the reputation of the profession.
The smart play, if someone goes down, is to ask if there is a nurse in the house. You are far more likely to get someone with the needed skillset.
Until the cops beat the shit out of said nurse. 🙁
A random person says “doctor,” they mean MEDICAL DOCTOR. It is understood. The fact that you have to CLARIFY that you are not a MEDICAL DOCTOR buttresses my assertion.
And the clarification is my point. Medical doctor alone is utterly meaningless. They mean a medical doctor trained in the field for which they need medical assistance. To go further, they don’t actually even mean that. They mean ANYONE who has medical training for that condition (nurse, paramedic, even a lifeguard with rescue medicine).
I think there is a widely held assumption that a medical doctor has the ability to diagnose and provide first aid to anyone. Tell the person asking that the available doctor is a radiologist, oncologist, etc and it will likely blow right past them.
The same assumption applies to us. I am constantly having to explain to people that I am a real estate lawyer and have literally never handled a criminal matter, not even a traffic ticket. They still keep asking for advice…
Yeah buddy, I took Crim Pro 20 years ago and spent the whole semester fighting with the Prof about mens rea and the evil of strict liability offenses. My advice is super valuable.
I have the longstanding opinion that lawyers are smarter than doctors
Some of the dumbest human beings I’ve ever met are lawyers. Going to law school did nothing to disabuse me of the notion that law school is inundated with moral defectives and very mediocre intellects who are able to bullshit their way into sounding smart.
*crosses fingers*
*mutters to self* please say present company excluded, please say present company excluded, please say present company excluded
Of course present company is excluded. Anybody who has survived the STEVE SMITH FOREST LAWYER CLE SERIES has shown mettle and moxie.
OT: 1 Reuben sandwich down. Will probably have another for dinner.
My fam does not appreciate the magic of that particular flavor combination.
Fuck a duck.
I’d prefer not to.
My dick doesn’t have enough spirals to make that work, sorry.
The complete lack of interest in the history and philosophy of law from all but a tiny handful of my fellow students really shocked me.
Going to law school did nothing to disabuse me of the notion that law school is inundated with moral defectives and very mediocre intellects who are able to bullshit their way into sounding smart.
Going to law school did much to disabuse my brother of his optimistic notions of humanity. He is now much more closer to being a curmudgeon like myself.
Holy shit, I had no idea how wokified doctor-school was getting. That is terrifying.
It is. The same tripe has spread into law schools. Maybe I’m out of touch, but if my freedom or property is on the line I want the best available attorney not the wokest.
Say what you will about Johnny Cochrane, the man knew how to try a case. He may have played off his race to get clients but once he got into court he was all business.
And, as a current MBA student, I can tell you it’s blanketed business schools as well.
Medicine and law chase fads just like every other occupation. No reason ever to think otherwise.
I took the MCAT in 1981 and of course it had nothing in it like that. The only weird questions were ones about how refrigerators worked, which seemed irrelevant and still does (i.e how do they work? You plug them in. That’s all I need to know, we have other kinds of experts to handle those concerns).
It’s reassuring to know I’ve had many pleasant years as a practicing physician before woke became the status quo, but even when I was in medical school there were outraged students who protested when some old guy (we had physician lecturers back then who were over 90 years old) ignorantly made a joke that sounded sexist. BFD, he was born in the last century, cut him some slack; nope, off to the Dean’s office to lodge a formal complaint.
I think like most professions, however, once most of these medical students get out in the real world they lose a lot of the school social justice indoctrination in exchange for common-sense approaches, at least that’s mostly what I’ve seen during my career. A lot of idealists become realists by the time they finish residency.
Look my good doctor, I’d at least like anesthesiologist to have a general understanding of the Ideal gas law .
(I’m assuming that was the ridiculous thinking behind that question. I’ll wait for Don and Yusef…)
I took the MCAT in 1981 and of course it had nothing in it like that. The only weird questions were ones about how refrigerators worked, which seemed irrelevant and still does (i.e how do they work? You plug them in. That’s all I need to know, we have other kinds of experts to handle those concerns).
It’s reassuring to know I’ve had many pleasant years as a practicing physician before woke became the status quo, but even when I was in medical school there were outraged students who protested when some old guy (we had physician lecturers back then who were over 90 years old) ignorantly made a joke that sounded sexist. BFD, he was born in the last century, cut him some slack; nope, off to the Dean’s office to lodge a formal complaint.
I think like most professions, however, once most of these medical students get out in the real world they lose a lot of the school social justice indoctrination in exchange for common-sense approaches, at least that’s mostly what I’ve seen during my career. A lot of idealists become realists by the time they finish residency.
Woke medicine seems like a bad, bad idea. They are bringing scientistic sounding ideas like “social justice” and holistic healing to a field that should at the very least Do No Harm.
Complex medical cases require knowledge from training, experience, and intuition from whereever, and a little luck to solve. I don’t want someone whose main aim is writing a social medicine paper instead of curing me.
I thought this might offer a break from the more serious stuff going on in the world, but feel free to immediately return to commenting on Covid-related hysteria.
Appreciated.
Seconded.
My rage receded briefly.
But you are still a rat in a cage?
That is in SUCH poor taste.
You are still impeccably dressed.
All our rats are free range!
Up to 93 deaths now after like 3 weeks.
Soon, the rest of us.
How many dead from car wrecks, cancer, drowning, choking, Drug overdose, etc in that same period.
Fake panic = power grab.
According to my local news, 0.
car wrecks
Around 2,600 probably.
I would expect those to be down. Suicide up maybe.
Finally more deaths than Ted Kennedy’s car.
But still far fewer than Ted Kennedy’s legislation.
And a thank you to the Editor for the great pictures.
I don’t think I would lean on the SJW stuff infiltrating medicine….seen what passes for Sociology or History lately?
As far as a using a title by education or profession…I’d rather we just not use them outside of a work setting. Heck, I don’t use any titles or letters in my correspondence, business card, etc. Why would I socially?
I would think, when one has such a powerful, narrowed gaze, the use of titles to establish hierarchy is rather unnecessary.
I’d rather we just not use them outside of a work setting
Pretty much this. I don’t call neighbors whoe are Doctors “Doctor” either. Only at the office of employment. Likewise I’ll call a professor “Doctor”, as that is what is common.
It’s when i’m working with the Doctorate in IT who is calling me for tech support and insists on being called Doctor, and if i don’t, she writes an angry note to my supervisor.
He’s Randy half the time. He’s Doc the other half, Gunsmoke-style. Both said lovingly for three decades. YMMV
Fair enough. I do call my freind who is a Doctor, “Doc” every once in a while.
Reminds me though of a Sales Manager at one of my jobs who went by “Doc”. I was really confused cause i knew there was no way he had a doctorate in anything other than snorting lines. Then found out it was his initials. D.O.C
oops: tone breakdown
I was just commenting along, not upbraiding
Don’t worry. I didn’t feel upbraided, was more issuing a slight modification to my own statement.
He’s Doc the other half, Gunsmoke-style.
Exactly what I call our Chief Medical Officer. Our uptight and somewhat insecure VP of Medical Affairs, also, although I can see it grinds her gears. Which is why I do it.
Had a room mate named Holloway, nick name was “Doc”
Besides the social and professional settings, there’s also the administrative settings. Things like dealing with local government bureaucracies. Credentialism is rampant but does help greasing the wheel for those things (e.g., homeschool application is most likely to pass through without issue if parents have advanced degrees).
My uncles is a physician who absolutely refuses to use his credentials in virtually any situation, which is the laidback kind of guy he is. He went with me to the ER when I had appendicitis and asked the resident all kinds of questions. The resident was kind of an asshole and started talking down to him before finally asked condescendingly if he was a physician or something like that. When my Uncle replied affirmative, the resident changed his tone immediately. It was interesting to observe, especially the arrogance of the resident and the willingness of my uncle to let it play out that far.
When my brother was in the hospital, he had to stop me from telling med staff that he was a pharmacist. “I want to see how much bullshit they’re peddling and they clam up when you tell them I’m a pharmacist.”
I do that a bit – I NEVER tell the other side in a contract negotiation that I have been a lawyer for 26+ years… until it will help me or my side.
Ambushes work.
The scary thing about the SJW stuff in the exams is that the “right” answers are either just opinions or demonstrably wrong.
Obligatory.
Step 1: Get Ph.D
Step 2: Call myself doctor
Step 3: Get chicks
You could follow the bloomberg method and skip all that learnin’ and just go right to getting chicks
Works for me.
Leonard Hofstadter?
FirstWife has PhD in nursing
My former mentor, an MD, has a husband university prof with a PhD.
She told me they had the nursing director of our facility back in the day over for dinner and he revealed to the husband he had a PhD in nursing.
Professor husband responded, “What did you do your doctoral thesis on, the proper use of bedpans?”
Apparently didn’t go over too well.
nursing isn’t widely understood, so he can be forgiven
FirstWife is a badass: BS/MS/PhD/RN/CCRN, operations admin, PALS/ACLS instructor, continuity of care expert, EHR deployment, EMT-B, organ donor advocate, community outreach evangelist . . . that’s just the parts that a mildly interested engineer figured out over two decades. She’ll die in the hospital she was born in, one way or another, really a great American if not a certain sort of warrior.
Patient advocate barely touches it.
Doctor is a boring title no matter who uses it.
Rex Catholicissimus. Now that’s a title!
Fun article, SSD! Credentialism has virtually zero place in my world but it’s good to get a peek into another!
King of the Universe?
So Dr. nurse?
I’m sure I saw that on Pornhub.
Ma’am, we need to check your temperature.
But we are all out of thermometers so we’ll have to use an alternate method.
Woo-hoo! I’m now Dr. Chafed.
What about the oldest profession?
Don’t they deserve the title, too?
“Noble Whore”?
Madam is a tilte.
That’s for management, elitist.
mistress for a certain subsection
“Madame” is a job description.
*sigh* I think I got “Madame” and “Madam” mixed up.
It depends on which Canadian province you’re referring to.
It depends on which Canadian
provincepolitician you’re referring to.FTFY.
Considering the care they provide to some of the schlubs who need it the most, I’m all for them having a title.
It’s a bachelor’s degree! It was always a bachelor’s degree until the 70s. My father still has the LLB and also has the letter from the College of Law offering to upgrade the LLB to a JD for a fee. It is a 3 year degree that does not in any honest sense require a prior degree. You have to have a bachelor’s to get into law school, but it can be in anything at all.
(yes this is a cherished pet peeve)
It’s a 3 year degree that should be 1.5 plus a semester internship.
*Thinks back to 3L course ‘load’ of Sports Law, Alternative Dispute Resolution, and Bankruptcy (because the professor was a hottie).
Yep. 1L is a serious year of school, add one semester to take some specific practice area courses and an internship to actually learn how things work and you have a better education by far.
My daughter’s ex-husband claimed he had 2 years Mech Drawing, 2 years Art School, 2 years Cooking School so he had the educational level as a PhD. He also lied a lot and couldn’t keep a check book. Called himself an engineer.
I’m lucky to have such an person, I mean really lucky that he’s my daughter’s ex. I believed he was Kreuger-Dunning. He made stuff up as he went along.
Kreuger-Dunning is under recognized.
I would argue that 6 total years of unrelated course work to be well under the achievement that a PhD is supposed to mean. A PhD should have focused specialty education and should be able to present and defend both a Master’s Thesis and a Doctoral Dissertation. Cooking school would help only in bribing the committee.
Lawyers have a doctoral degree. We should have the same right as a Ph.D. to demand that people call us “doctor”.
In a hospital, of course, calling anyone but an M.D. or D.O. “doctor” is a massive faux pas, so I don’t have to deal with Ph.D.s demanding unearned respect, just M.D.s and D.Os.
In one moment of supreme crankiness, I was at a gathering where some Ph.D. snottily “requested” that I use his title. I told him I would call him “doctor” if he returned the courtesy, as I, too, had a doctoral degree.
In a critical tactical error, thinking he could bump uglies with me on credentialism, he asked where I went to law school (pixels can’t convey the sneering contempt). I told him “Harvard”, and suddenly the credentialing competition was called off.
In fairness, I think using the title is fine in settings where it is relevant. In a hospital, being an M.D. or D.O. is relevant. In academia, being a Ph.D. is relevant, so I got no problem calling a Ph.D. “doctor” when I am on campus.
I thought lawyers weren’t Drs until they got their JSD or SJD?
Nope. The degree conferred after three years of law school is Juris Doctor. Nobody uses the title, although annoyingly I see more and more lawyers putting “J.D.” after their name.
It was always used only on official correspondence, when you were writing as a lawyer. I used it briefly when I first started (old-school law firm in Richmond, VA), and then I figured the law firm letterhead probably gave people a clue, and stopped using it.
“Law firm letterhead but not Esquire? Either a paralegal or legal secretary.”
Old school law firm in Richmond? Which one?
Hunton & Williams.
Oh, the behemoth. I know a few of their lobbyists.
Huh.
Three years of Law School in Canada gets you the “LLB” designation (roughly, “Bachelor of Law”). Mucho additional study gets you “LLD” (“Doctor of Law”). ”LLB” makes sense to my mind, becuase it’s still possible to gain admittance to Law School in Canada without completing a Bachelor’s in something else first (you can be admitted with just two years’ worth of a four-year undergrad). I actually knew one guy who never went to Law School at all — he articled for several years with a lawyer and then sat the Alberta Bar exam. Presto, he became a lawyer.
When my grandfather went to law school, he just had to pass a test. I don’t think he went to college.
At what point did a formal legal education start to be a requirement of sitting for the bar rather than learning the law via an apprenticeship to a lawyer?
When Herr Doktor Professor Esq wanted to reduce the number of uncredentialled lawyers showing him up.
It always cracks me up when I get a letter addressed to “[informal nickname], Esq.”
Now I need to find a way to use the character of Bubba Jack Esq.
Engineering Economics was taught to me by a lawyer; we saluted him with the full “Doctor.”
At the end of the day, that was as important a course as I have ever taken.
“Engineering Economics…”
That and Technical Writing were probably the two most worthwhile courses I took to get my engineering degree.
In a hospital, of course, calling anyone but an M.D. or D.O. “doctor” is a massive faux pas, so I don’t have to deal with Ph.D.s demanding unearned respect, just M.D.s and D.Os.
I can’t speak to hospital staff, but I’ve never heard of PhDs not being introduced as Dr. so and so at any medical device presentation given at a hospital or medical conference. And I’ve prepared many of these presentations for hospitals and medical conferences all over the country. Of course, it’s first names after the presentation with no formal title or last names period.
it’s first names after
I badly miss the respectful distance. The world is business casual anymore, but I’m not convinced that this familiarity breeds efficiency.
/ Southern dinosaur, nearly extinct
Law is still like that.
Same here. I call M.D.s “doctor” at work even if they also go by their first name. I also call normal people “Mr.” and (yes) “Ms.” at work until they ask me to use their first name.
“That’s Mister Firstname“
presentation given at a hospital or medical conference
Or steak houses of course. Forgot to include that popular one.
I despise credentialism.
The fact is I have far more respect for you RC because of the things you have said and taught me over the years than I would because you have letters after your name. I would call you by your proper name and my respect would be clear from my tone and behavior.
Anyone demanding to be called Doctor would probably just get a middle finger from me.
Proctologist Dr. Suthenboy.
Suthen!
Feeling OK, I take it?
How many fingers am I holding up? ?
I look like shit but I am ok, thank you. Headache gone, vision normal. Wife quit fussing at me.
The funny thing is the little dog is housebroken and I blame myself for having one too many and falling asleep letting him go too long between outside trips.
I despise credentialism.
#metoo
*Resumes work on earning Project Management credentials.
At this point in time, in contemporary American society, what exactly does “marginalized” even mean? Who is marginalized? For example…..almost every movie and TV series these days has at least one gay character. Sure, it’s often shoehorned in for no apparent reason as a token – like in the Netflix series Messiah that I just watched, a major character is revealed to be gay in his last appearance of the season in a brief scene that has nothing to do with the plot. Still, they’re there.
TV advertising requires mixed couples, otherwise someone will be othered
And the mixed couple is almost always a black woman with a white or Asian man, a pairing that is exceedingly rare in real life when compared to black men with white women or white men with Asian women.
I used to work with a gorgeous black lady. Her boyfriend was a skin-headed, pastie white dude with lots of tattoos. They used to get double takes all the time.
Why does the Pornhub algorithm have to be based in reality?
Libertarians.
I’m pretty sure they run the country along with (((them)))
They don’t count because they’re horrible people who deserve to be marginalized.
I’m going to take the unpopular position here that PhDs have just as much a right to the Dr. title as physicians. – in a professional setting. I aint calling a physician doctor outside a hospital/clinic
For full disclosure, I am working towards my PhD now, but this has been my inclination since well before going back to school. – lame. or gay. or nerd. or something.
The captain has turned on the Fasten Seat Belt sign.” Here we go again. Who gives a shit who turned on the sign? What does that have to do with anything? It’s on, isn’t it? And by the way, isn’t it about time we found out who made this man a captain? Did I sleep through some sort of armed-forces swearing-in ceremony? Captain, my ass, the man is a fucking pilot, and he should be happy with that. If those sight-seeing announcements are any mark of his intelligence, the man’s lucky to be working at all. Having endured enough nonsense from this so-called captain, I finally raise my voice: “Tell the captain, Air Marshal Carlin says he should go fuck himself!”
*applause*
Carlin’s airline bit is one of my all time favorites!
“You don’t take a shit. You leave a shit!”
“Finally, the last argument is that if PhD can use the title “Dr.”, what about those with doctorates? I don’t know, the rapid growth of doctorates is a recent phenomenon and goes hand in hand with the above credentialism point. PhD programs are much more rigorous than a doctorate”
OK, gotta admit this one took me by surprise. What are some examples of earning a doctorate outside of a PHD? When you write “rapid growth of doctorates” I assume you’re referring to something other than LL.D. or JD.
What the hell is an LL. D?
Googles: Wiki:
In the United States of America, the LL.D. is awarded as an honorary degree only. The terminal academic law degree is the Scientiae Juridicae Doctor (S.J.D. or J.S.D.), equivalent to the Ph.D.
ahhh ok.
I’ve never even heard of an S.J.D., even on law school faculty. But I don’t have much truck with academics, so maybe I missed it.
LLM?
Credentials creep. Hell, positions that didn’t used to even require a BA now are Masters “preferred”.
I get that. What I’m trying to figure out is how you earn a doctorate outside of a Ph.D. program (obviously my own biases are at play here).
“Dr. Jill Biden”
^This. One example is physical therapy. Formerly only needed a masters but now need a doctorate to practice if not grandfathered. Doctorate program is the same as the Master’s but costs more. So, in addition to the credentialism, it’s also about more money for the accrediting organizations.
So, you can earn a PhD – or is it a doctorate – without having to produce any kind of original research?
I believe it’s a doctorate. No original research.
Well, someone has to pay for all those diversity department staffs and vice-deans of equity.
Various “professional degrees”, other than MDs and JDs, we have Doctors of Business Administration, Ed.D.s (which predate Ph.D.s, I believe), etc..
Ah, of course. I guess I just assumed you had to write some kind of diss for an Ed.D. Don’t know why I assumed that.
Checking the history, it turns out I was wrong. Columbia offered the first Ph.D. in Education in the late 19th century and Harvard offered the first Ed.D. in the 1920s. That having been said, I know several Ed.D. programs that are research based and require a dissertation, so you can’t always judge based on the degree.
In fact, if I’m having a health emergency in public, I’d much rather a paramedic step forward to help than a psychiatrist
I dunno about that. *SSdad collapses, clutches chest* “How does that heart attack make you feel?”
I once had a podiatrist try and give me direction on a vehicle accident. I handed him the card from the county EMS with micro-type on it generated for just this type of situation. He looked at me in disgust and walked away.
“First, check for bunions…”
Look Fats, I didn’t spend 5.5 years at The Ohio State University almost earning a four year degree just to be called “Hyperbole” (or even worse “Hype”) by you assholes. It’s “THE Hyperbole” godammit! “THE Hyperbole!”
Look, a regular bole.
Woah Woah Woah. Did you just lump us into a collective of Fats? That is seriously hurtful.
I’m feeling marginalized.
No, you mean Margarineized
Soooo… ‘Lacist!
A fats of glibertarians, has a nice ring to it.
My dad has a doctorate in Geography. Useful for teaching overseas – and I think in a professional/academic setting/conference/etc it makes sense to refer to them as Doctor (shorter than ‘Professor’ too). Outside of that, not necessarily an issue.
“Herr Doktor Professor…”
and his wife Frau Doktor Professor.
People refer to me as doctor sometimes, but only because I’m a doctor of love.
I prefer to be called by my first name, even by little kids. Over the years I’ve been called a lot of different things, often by my wife.
You just told them to call you whatever they felt like cause it was no skin off your back, but not to ever call you late for dinner, right?
Same here. Even my grandchildren call me by my first name. Various others have called me by lots of colorful names.
Update: Costa Rica has banned all incoming flights starting tomorrow. Conference is canceled after today. Talked to a Spaniard and he says he is debating staying in CR, because spain’s infection/death rate is skyrocketing. People over 60 in Spain are being denied treatment for COVID-19. All elective surgery is canceled starting tomorrow in my system. Tent city erected outside of my hospital. All people screened before entry allowed into hospital.
Please remain calm. If you are under 65 and otherwise healthy, you are NOT at high risk for adverse outcomes.
I’m more annoyed at the overreaction than anything else.
I’m annoyed by the over reaction. I may get trapped here if there are no incoming flights. I have no idea if there are private planes for charter and I have no experience in chartering one.
Are you in the Liberia or San Jose area?
I flew into LIR.
Charter costs are probably going to be in the $50K range to the US for up to 16 people.
Evojets.com
Wow. I had no idea it was that expensive. Even if I can split it 4 ways that a tremendous price. It would be cheaper to stay at the resort until flights resume.
Yeah, it requires a long range jet.
There’s going to be some private flights out for certain companies (Intel has a facility in Heredia), but I doubt they’re going to share.
Your best bet may be to contact the embassy and get advice.
Take a bus to Panama? I think the airport there is a little larger – or you could maybe catch a ship….
Ask the embassy?
That’s good advice. Thanks.
There’s an international airport in David, which is close to the border.
Just hitch a ride with one of those Soros organized migrant hoard trains.
I giggled
Update: Costa Rica has banned all incoming flights starting tomorrow.
And they are going to stop them with what Army?
lol. The U.S. army I guess, since we’re responsible for their defense.
Last I checked, the CR police carried Uzis and rode dirtbikes. It’s like an Army of Chuck Norris’s
They’re going to switch of the ILS transmitters and scatter caltrops on the runways.
30 Ticos with slingshots.
The police and the jungle are are their army.
I *still* want to know what the actual hospitalization rate in the U.S. so far. This is information that will easily let me calculate how serious this is, and I can’t find it anywhere.
I’ve been following the tracker out of morbid curiosity: https://www.worldometers.info/coronavirus/ (they’re all different, so who’s to say this one is more accurate). The good news is as the deaths come in here in the U.S., the mortality rate is dropping. Getting close to 1.6% now. I suspect we’re still missing over half the population in the set because they are accruing very mild to asymptomatic cases.
I’m 90% convinced I had it, but have not been tested.
I too had all the symptoms absolutely perfectly about a month ago, but it doesn’t fit the timeline they’re giving.
Mine was a week ago.
I Dont know if you’ve visited this site:
https://coronavirus.jhu.edu/map.html
That one is like 800 cases behind the other site, but no idea which one is more accurate.
I think jhu and worldometers use the same data, they just have different intervals for updating the data, so you will see some discrepancies. I find worldometers easier to read for country level data, but jhu allows you to drill down more.
I suspect we’re still missing over half the population in the set because they are accruing very mild to asymptomatic cases.
Seems highly likely.
Utah Jazz star Donovan Mitchell says ‘scariest part’ of having coronavirus is that he has no symptoms
very likely
A Romanian guy in Spain was diagnosed with the virus but had relatively mild symptoms and was not hospitalized but had to quarantine for 14 days. This did not suit him he decided to return to Romania so got on a plane. How this happened is unsure, but there were 60 others on that plane.
Similar story in the U.S. last week. A dude was mildly ill and got the coronvirus test. Then he hopped on a plane. While in transit, he got the message that he was positive. So he got to stand up and tell the plane they might all be infected.
That wasn’t the guy who was just joking about it and got arrested for it, was it?
I don’t remember seeing him being arrested and I don’t think he was joking.
I think the worst part is he traveled out of JFK. Who knows the number of people he was next to.
I think Urthona is talking about the guy that earned a lifetime ban from JetBlue.
I am unsure how quarantine would work in libertopia but I assume some people getting a beating would be involved.
We have an example of sorts. A 53 year old man who tested positive in Kentucky left quarantine in the hospital and went home. The cops have surrounded his house so he doesn’t leave.
He should go outside and breath on them. Are they gonna shoot him?
I wouldn’t be surprised.
*sigh*
You’re asking if a cop would shoot him? That’s not a serious question, is it?
^^ way scarier than a fucking virus^^
New Zealand is detaining and deporting foreigners who fail to self-quarantine on arrival.
Singapore has been revoking residency cards for non-citizens who don’t follow stay at home orders.
There is a definite part of me that wonders why we just don’t quarantine the people who are in actual danger only, which is why I want to look at the real hospitalization rate.
That was one solution offered. Quarantine people over 65 for two weeks and everyone else continue as normal. Gain herd immunity then let’s the olds outside.
It would take longer than two weeks to spread to everyone.
air, another tragedy of the commons?
I barely stumbled back into the house after taking the trash out this morning. It rained somewhere an inch too much, and now Yankee turds are floating by . . . and it was a very , very bad day for somewhere upstream. I’m used to a NYC-grade stench for a few hours about once a month, but today I’m getting hammered. How about a courtesy flush: flatten the curve for us down here!
You want to be involved in our public activities? OK, then agree to stay the hell away when you’re sick.
Deal.
or
No deal. In which case you aren’t invited to stay.
Yeah, one of my colleagues (who is pretty left) suggested the same thing here for St. Patrick’s Day. You want to go an drink in a bar with 200 people, you go to the back of the treatment line. Of course, then the governor banned gatherings of more than 10 people.
We heard about a woman whose husband was hospitalized with Kung Flu.
She came to visit him every day in the hospital. While she was under home quarantine. What a fucking idiot.
Our understanding is that the hospital called the County Health Department, who called the sheriff, who had a chat with her.
Here’s a Dr. for Mo.
My apologies to the rest of you.
YAAAAASSSSSSSSSSSSSSSSSSSSSSSSSSSS
I knew what it was before I clicked.
I saw them on the Dr. Feelgood tour. I wouldn’t have been able to, but the mother of a couple of teens in my karate class paid for my ticket if I’d drive from Provo to Salt Lake and chaperone.
*I* was the one who got in the fight, though.
??
Another doctor for Mo
You guys should just do it our way. From Karate masters to teachers to doctors to oddly named commenters, it’s “Sensei”.
No.
Sumimasen UnCivilServantSan.
für acht Jahren: Herr Doktor
Thank you, thank you very much…
It’s actually how I do refer to my Japanese teacher and becomes second nature, doesn’t it?
Also not attaching -san to most people’s name seems odd.
But isn’t Sensei-san a bit much ?
But Sensei-chan seems a little odd.
My opinion on Doctor title. Use it at work, leave it at work. Sorry to OT.
Pithy, and correct.
Titles.
Reading and writing historical novels that involve officers who are also nobility has had me confused for ages and although I THINK I did it right in my pirate book, I can’t be certain.
Admiral Lord Hylton.
Good heavens. That seems exactly backward to me.
========
Unrelated: My 75yo mother is rolling her eyes at this and as irritated as I am about how overblown and inconvenient it is.
A Lord Admiral is a higher ranking naval officer, Admiral Lord Soandso is a Lord who also happens to be an admiral.
aka Commander in Chief (of the Navy).
Nobles don’t “happen” to be officers. Nobles are de facto officers.
In Master & Commander, they had a kid (12? 13?) who was [Officer Title] Lord Whatever. He was a go-getter, though, and gave good commands. He lost an arm.
Not all noblemen went into the service.
And aside from being press-ganged, it’s hard to ‘just happen’ to be part of the royal navy. Besides, the press-ganged don’t get to be Admirals.
I didn’t say they did, but I also didn’t specify that those who did were automatically officers.
Re noblemen: “First to heir, second to military, third to the church.” (Or law.)
And my “happens to be” happens to be a quirk of verbiage.
Yes. At that time, most (maybe all? I don’t remember) commissioned naval officers were noblemen. That’s why warrant officers were created – they were technical experts with much experience and specialized knowledge who were from humble backgrounds and thus not considered gentlemen who could receive a commission.
Never forget that officers in the US uniformed services are gentlemen by Act of Congress, not necessarily inherent.
Also, they could not pay for a commission. Officers bought their positions, at least in England until sometime in, I think, the late 19th century. Creating “warrant” or “non-commissioned” officer roles was the only way to put their expertise/abilities to good use.
I don’t think the US Army ever sold commissions, but I could be wrong. At least in the Civil War, a lot of people with zero military experience stepped into officer roles, including high-ranking officer roles.
The purchase of commissions was abolished after the Crimean war.
*in the UK.
In the US, I’m pretty sure if you raised the regiment, you could be colonel.
Purchase was an army phenomenon. I don’t think the navy used it, or if they did they got away from it much earlier.
Yes. That’s how Nathan Bedford Forrest went from a private to a lieutenant general over the course of the war – he was a rich man, raised his own regiment, and paid out of his own pocket to equip it.
There was at least one case of a pressed man rising through the ranks to hoist a flag. I don’t remember the name, but I remember reading the story at some point.
Andrew Mitchell?
Who you calling a civilian, civilian?
As always, few topics fail to remind me of some policestuff outrage
I love when they are even dumber and refuse to call cops Citizens.
Reporter just asked Trump about saying “Chinese virus” because the term creates a stigma. Trump said “no, I think claiming the US military gave it to them creates a stigma.”
Dammit Trump! Stop making me like you!
+1 – That’s great!
Next thing you know Trump will inter Chinese Americans in order to quarantine them from the rest of us.
We will bury them! [pounds shoe on table
The Ghost of FDR smiles.
Our oldest is working gradually on her Doctorate in Practical Nursing. As such she’ll be entitled to call herself “Doctor.” But having a nurse use that title really gets MDs riled up.
Which means, of course, that she will insist on being addressed as “Doctor.”
In this case, I think she should. Because it pisses people off.
Which is why she’ll do it.
See if she wants a direct commission into the Navy Reserve too. She’d start out as at least an O-3 and only 2 weeks in Rhode Island instead of the full 9 weeks of OCS crap. Good bonus and incentives too.
She’s too old; she’ll be 38 in May.
Medical and direct commissions (like Chaplains, etc) have tons of exceptions in the reserves – as long as you’ll hit 20 years before you turn 60 (some even after that).
Yeah, she still isn’t interested. She was turned down for the Air Force Academy years ago due to being deaf in one ear, but mostly, she’s very happy with her life in her little Iowa town and isn’t anxious to change anything.
That doesn’t make sense. You said “she”, right?
Which means, of course, that she will insist on being addressed as “Doctor.”
I would advise against, as this will be a severely career-limiting gesture.
She runs an ER in a tiny farm-country community hospital in eastern Iowa; her career is already about where she wants it to end up, so she’s not terribly worried about that.
My preference for primary care is NP’s or PA’s. They seem to have it more together for routine stuff.
Trillion dollar stimulus, and $1000 checks mailed to everybody in a couple of weeks. Hallelujah, the economy’s saved.
“We have to do something about inflation”: politicians in about 6 months.
The have never ever cared about price inflation. They only ever cared about the inflation of loan interest rates.
SNORT. as if
We just got Yang Ganged.
dilution is the solution
Unless that 1000 bucks is prorated for race and gender, I find it highly problematic.
Great. The price of bribes just went up.
The price of
bribesganja just went up.At the end of the month, the same six guys as always will have all of it.
I’ll take it.
I’d take the long view and say fuck you, cut taxes, but that will never happen and I am a pragmatic sort.
At least they delivered it in cash when they did that with ISIS.
Right?
Come to my house and put 10 Benjamins in my hand.
We already got something from the govt here. Everybody with kids got something like 8000 yen/kid. Something like that. Ooooh, thanks for the $75 dollars as I pay $5000 in taxes.
Don’t remind me that I just filed my taxes this week.
Yeah, I gotta finish my taxes this week. I make less than $15/hr and NYS is taking over a grand from me in income tax, never mind SDI or the family leave tax.
Yep, said it yesterday it’s all pretend money anyway, they’re just going to print more and hand it out to their cronies and the like, may as well get everyone in on the graft. If it brings the whole charade crashing down so be it.
We all know how this game is going to be played:
1 for you; 1 for me.
2 for you; 1,2 for me.
3 for you; 1, 2, 3 for me.
Cool, a grand to spend on ammo.
We were bullshitting this morning before a meeting on Kung Flu about the panic. I told them I was going to panic-buy some ammo. The reactions were amusing, since our team is about 80% Dem drones when it comes to politics.
“This is why we need to close Gun Shops till this emergency is over”
:Narrator: The emergency was never over.
I hope the census mails the checks. I got THREE envelopes from them over the last 4 days.
The last time government did this ($350 Bush tax cut) banks went apeshit months later as people paid down debt thus exposing the fraudulence of the banks’ “tier 1 assets.”
Pretty neat article about smallpox in the blankets.
https://www.historynet.com/smallpox-in-the-blankets.htm
For folk who work at those take-your-pet-to-work places:
what expectations do your employers have while your dog WFH ?
Mine’s napping. Same as when I take him to the office.
Mine’s vigilantly guarding the house from mailmen, as he does every day.
I think the issue isn’t whether or not a certain individual deserves a title, but that society at large worships at the altar of Presumptive Immortality, and MDs are the priests of this civil religion. To call someone not initiated in the holy rites by the sacred title is blasphemy. This goes hand in hand with two other modern societal trends; the first being that academics, and to a certain extent, lawyers and non-clinical medical researchers, are members of “expert” professions, in which status is accrued based on what you know, not necessarily what you can do. This runs counter to the mentality that is glorified in business and engineering, especially, in what you do is all that matters. NotAdhan wrote an article from that perspective concerning “bullshit” jobs. The ever-present strand of anti-intellectualism in American society is woven with the current strand of populist egalitarianism. In the past decade, a curious case of Tall Poppy Syndrome has infected our society and anyone seen as too “uppity” is socially punished. Self-styled “deplorables” loathe the idea that anyone might think themselves better than they are based on income, education, social status, region, etc.. They are correct, in a way, however, it too often spawns a preemptive sort of radical populist egalitarianism impulse that is the same exact impulse that caused communists to force everyone to call each other “comrade” upon pain of death.
Thesis begets antithesis. In this case, metastasizing credentialism begets radical populist egalitarianism. Which is appropriate, as credentialism is increasingly used to guard the class barricades against the unwashed.
I agree. When I wrote “In the past decade,” the year “2008” was firmly in my mind. The excesses of Obama’s technocracy fertilized the excesses of today.
Fuck you, asshole! You know I can’t understand that fancy talk!
What I’m trying to say is this.
Interesting. I’d agree with you on the “Presumptive Immortality” part. Talked with my wife about that the other day. In life getting sick and dying is the standard. The fact that we have gotten rich enough that this rarely happens is a great thing. Saying that it should never happen is a pipe dream.
Interesting on the flip side however is the American Religion of Public Education. Not a lot of titles are lauded or money, but you’ll be damned if you don’t pay lip service to Valiant Mrs Third Grade teacher.
Rogers Hornsby 0.359
Ty Cobb 0.366
Father Time 1.000
Don’t forget “Thank you for your service.”
I rather would.
I haven’t met anyone who likes that.
Around this guy’s funeral, a bunch of military folks were hanging out in a local bar. I was sitting near them.
Two guys and two women. The one woman was married to the one guy. I am not sure, based on what I overheard, if that woman was in the military. The other woman and both men were current military.
The military woman was eating up the fact that the locals were thanking her for her service, calling her a hero, paying for her drinks, and paying for her food. She loved it and was going on and on about how wonderful the locals were. She was loud enough that I’d say half the bar could hear her, and yet people were still approaching her to thank her for her service.
One of the military guys was embarrassed by it all. I overheard him say, “Why do they think we’re heroes? We really don’t do all that much.”
I can’t stand it. I wish I hadn’t gotten veteran on my license, but I thought it might save me a ticket or two. I don’t want to be thanked in the grocery checkout line, or every fucking where, for the fact that I entered into an agreement to join the military. My stock reply, not snarky, but matter-of-factly, is “Oh, I volunteered, but I was paid. No thanks necessary. I’m not sure I would have done that for free.” That’s usually enough to end the matter and we can all go back to our lives. I know people mean well, but it all feels like another form of virtue signalling. Everyone loves the military now and it’s gauche not to; I remember when no one had yellow ribbons on anything and no one gave a fuck if you had served. I take it with a grain of salt – it’s nice when people are nice, but when there was a draft, the American public collectively showed what it really thinks about compelled military service. I think a lot of it is guilt expiation – the American people like – and want – a military that is second to none and they’re willing to pay for someone else to shoulder the burden. ‘Cuz they sure as fuck aren’t interested in humping a pack, or going on deployment, or leaving their families, etc. And it’s part of why our foreign policy is so fucked up from both parties. The actual people who have to eat the shit that is US foreign policy are only a miniscule, dispersed part of the electorate. When everyone’s kid goes, it’s a whole different kettle of fish.
I agree with HM and only change one word – “Presumptive Inerrancy” vice “Immortality” – only because I’ve not heard that phrase and don’t know what it means. It strikes me that credentialism is explicitly a part of the post-Modern milieu, so much so that credentials, “peer review” publication, and other indicia of Ethos (of the Ethos, Pathos, Logos of all argumentation) have replaced entirely the substance, the actual res, of knowledge. We have a shit-ton of the appearance of knowledge, and the store of human knowledge at our fingertips, yet we certainly don’t appear wiser, in any measurable or quantifiable sense.
“….status is accrued based on what you know, not necessarily what you can do. This runs counter to the mentality that the glorified in business and engineering, especially, in what you do is all that matters.”
I subscribe to the latter but there is a bit of crossover. The problem of course is that there are a large number of knowers that cannot do and they give the ones that can a bad name.
Fun show….The Riches. Complete con artist, bullshitter pretends to be a lawyer yet knows nothing about law, still he becomes successful and rises to run a 100M+ company. We watched it on Hulu.
The thing is that in both my academic position and in my small consultancy business, people pay me for what I know. What they choose to do with that information is up to them. Now, the knowledge I have accrued comes from my previous time spent doing shit, but as it stands now, my knowledge is my meal-ticket. As such, all the letters in front and behind my name are marketing tools more than anything else – placards hung outside my “door” to advertise.
Deserves what a bad term. Good point. I often read that thrown about in the threads so added it here.
*Deserves IS a bad term. Can’t type for shit today.
Is THAT how rights work?
Very nice.
Only the good rights, like the right to an income and the right to health care. Not bad rights, like guns and free speech.
Good rights = rights that allow looters to wet their beaks. Any right that empowers you as an individual is yucky.
You made my day. Thanks.
Well, in all fairness, I can’t think of a better way to make guns unaffordable and inaccessible than by having a federal program to ensure that every American can own a gun.
News you can use: https://www.fox29.com/news/dont-drink-bleach-to-prevent-coronavirus-poison-control-center-warns
voluntary tweaking of the gene pool that doesn’t take out any innocent bystanders is okay by me
That’s kindly referred to as mountain medicine.
It needs a better euphemism. How about traditional country medicine or TCM?
Call JG Wentworth!
Hmph.
The hospitality industry basically cancelled my vacation, so I’ve got everything I saved up for a two-person road trip.
Ill be changing my name to Doctor Tres.
Doctor Reverend Tres!
https://whotv.com/news/gov-reynolds-issues-a-state-of-public-health-disaster-emergency/?fbclid=IwAR1VhqfodabYOh6V89i3cn04xBZYJFQ2lHZZ232jQbkUNit_3D8hR8YrgZM
DES MOINES, Iowa — Gov. Kim Reynolds has issued a State of Public Health Disaster Emergency that goes into effect Tuesday, March 17th at noon. It lasts through March 31st.
It takes significant steps to require social distancing and limit community spread of COVID-19.
This requires closing restaurants and bars to the general public, although it allows carry-out, drive-through, and delivery. Fitness centers, health clubs, gyms, and aquatic centers are closed, along with theaters, casinos, and gaming facilities. Planned large gatherings and events of more than 10 people must be canceled or postponed until the public health disaster is over.
Fuck this nonsense.
Republicans for Freedom™
Minne announced it yesterday
10 days.
What the fuck will 10 days do?
Can I go outside? And can I go outside to go? We’re right on top of things here. In 2 weeks all the deplorables will be fed up with the restrictions and want to go somewhere-anywhere, burn up some of that cheap gas (1.79). Sit outside on the deck and drink, coffee for me, whatever else you chose.
In 2 weeks all the deplorables will be fed up
Nobody who matters cares what the deplorables want.
Except for the fact that the deplorables have the guns.
let ’em drink bleach
The street cleaners are out here in Amesm this is the fourth pass on my very clean, deserted, street – – banking that sweet OT.
A lot of this crap is coming straight from that buffoon Fauci (Dr.) – if this guy had been appointed by Trump, everyone would be calling him out for the moron he is. At this point, he is the one person Trump can’t/won’t fire.
Thank you!
I thought I was the only person who couldn’t stand that smug asshole.
Promoting from deadthread:
Here’s the deal on flattening the curve and the capacity of the US healthcare system:
The system is built to manage a bad flu season. We have them periodically, and we manage them (with some stretching and pain). If the Kung Flu was going to peak during a peak of the flu season, that would be bad and would overstress the system.
But its not. This was a typical flu season, and is already on the declining side of the bell curve. Kung Flu will peak after the flu season peaks. Assuming it is no worse than a bad flu season, we will have the capacity to manage it. Worst case scenario is that Kung Flu requires more negative pressure rooms (which you can be convert a normal room to; its an exercise in HVAC engineering) and respirators (which the CDC has a stockpile of).
Some curve flattening is a good idea, but you get the most bang for your buck by closing borders. Keeping patient zeros out has disproportionate benefit to trying to control an epidemic once it has a foothold. The stupid lily pad analogy points the way – keep the fucking lily pads out of your pond – but nobody gets it. In any event, we are past the point where border control has the maximum impact. Certainly no reason to import more, of course, but its here now.
As testing spreads rapidly due to the efficacy of a private lab industry, the number of confirmed cases will skyrocket, feeding the panic and pointlessly compounding the damage.
The system
the System?
Your ever-changing handles and avatars give me a smile.
schizophrenia FTW !
I don’t even remember what the first avatar was
but I used Escaped at TOS
How do you know we have the capacity? The actual data on this is no where to be found. I strongly expect we do, but there’s no way to know.
How do you know we have the capacity?
I know we have the capacity to manage an outbreak of serious communicable disease on the scale of a bad flu season, because we have done so repeatedly. Flu puts peak demand on hospitals (and the health care system generally) every year.
As I mentioned, its possible that Kung Flu will put more pressure on certain resources (negative pressure rooms and ventilators) than the flu, but those resources have room to expand.
The other variable is sick staff, but this is also an issue during flu season. Its possible that Kung Flu will take more staff out of circulation, which will put pressure on capacity.
except this spreads much faster than a serious flu and is anywhere from 5 to 10x more likely to require serious treatment. Supposedly.
Is that true, though? I’ve heard wildly varying numbers for SARS 2: Pneumonic Boogaloo’s R0. We need more n, as always.
I’m reading 2.2 R0 for this and 1.3 for serious flu, but OF COURSE I have no fucking idea.
I am strongly suspicious of the data coming out as I am of all things.
But if you *believe* the data, is believing that the hospitals are in trouble that much of a stretch? Perhaps not.
Just a few days ago, it was being publicly stated that Rₒ was in the range of 4.0 or thereabouts — I see that a few days’ extra info has revised that downwards. Interesting.
Transmissability is one thing, and it looks like the Kung Flu is likely more transmissable than the regular flu (although they are both “droplet” transmission, we think, Kung Flu seems more infectious). Again, though, what’s the bias in the data? Flu is pretty normalized; Kung Flu is not and will be tested for at a level we don’t test for flu – the same “real” transmission rate will show up in the data as Kung Flu being more transmissable because we have more tests that will show more mild or asymptomatic cases. Nobody test for asymptomatic flu, and even mild flu cases aren’t tested all that much.
Severity is another, and what drives demand for hospital services. That’s the number we don’t have good handle on at all. Everyone has some resistance to coronavirus generally; we’ve all had mild infections from it that were passed off as colds. How will that play out? Nobody knows.
Assumes facts not in evidence.
You can’t generalize from terrible Chinese hygiene and impaired respiratory systems, or petri dish cruise ships, or an elderly Italian population and undersized hospital system, to the American general population.
I think the best “front-runner” for the US is South Korea. I’d keep an eye on data from there if you want an advance look at infection and mortality rates. Japan, which is much more urbanized than the US, may not be as good a comparator.
Assuming that the worst case scenario you describe is what actually happens here, then we’re fucked anyway without all this nonsense about flattening the curve. The worst-case scenario would overwhelm our curve-flattening measures pretty easily, unless we go to full lock-down, nobody allowed out of their house except for once-weekly trips to the grocery store.
In short, if this thing really has 10x transmissability and 10x mortality compared to the flu, then nearly everyone will catch it and 5% of us (17,000,000) will die, regardless of curve flattening. Of interest, that was pretty much the worst-case mortality scenario for H1N1, and was off by orders of magnitude.
Didn’t South Korea start giving people chloroquine pretty early on?
On a related note, this better be the end of Certificate of Need nonsense. If there is any question about capacity, then every fucking hospital ever proposed was actually “needed”.
Not that that is the reason to end those laws.
What’s disappointing is that most people don’t even know those laws exist.
Every time someone claims that the free market “just doesn’t work for healthcare”, I tell them about those laws. They’re always shocked and agree that those laws need to go… But it never seems to sink in. I can talk to them a week later and they’ll still be back on the same tangent about how American healthcare is fucked up because of “unfettered capitalism”.
They’re a particular bane in Virginia. The committee that decides on CONs is controlled by the existing healthcare players.
My entry into hospital law was to manage a new CON statute for Wisconsin hospitals.
Instead, I pushed for them to repeal it. Which they did.
Of course, they still pay the tax to fund the CON agency (thirty years after repeal).
I’m curious whether you see positive rationales for CON statutes?
I’m going to start using the term “unfettered socialism”.
i bet the socialists would get in a tizzy fast if you did.
Doesn’t take much to get socialists in a tizzy.
Yet you know that in fact it will more likely be used as an excuse to make CoN laws more stringent. Can’t trust our healthcare to just any start-up hospital.
In case you were wondering…..yes, government apparatchiks are giddy over the possibilities their new powers present to them, as demonstrated by some USDA drone:
Randazza is a rock star.
The USDA should very publicly can his ass.
Apparently he’s not an employee. Just another fucking Internet tough guy who is a master of gorilla warfare.
*insert HM copypasta here*
well, I’ll be a monkey’s uncle
#MissingGramps
Take a wild guess which department’s employees would be the first to hang from the nearest lamppost with their remains gibbeted as a warning to other departments?
?
I don’t know, but this guy should be hanging now.
Federal food rationing will lead to dead pubsecs, I do believe.
That type of honesty is refreshing.
They don’t have any new powers.
The more this goes on the madder I get.
Cant gather more than ten people you say? Fuck you. Go sit on a sharp stick. If you need help picking one out I can give you a hand with that.
You’re right. The EOs they’re going to cite were issued during the Cold War. No one did anything because they were hoping that when they had to pull the trigger, their team would be in charge.
I can’t belive I’m the first to post this. Doctor, Doctor, Doctor, aaannnndd doctor.
https://www.youtube.com/watch?v=hoe24aSvLtw
Doctor! Doctor!
Re topic: I wish we had equivalents of tutoyer and vousvoyer in English.
Thou art in luck. You can have your wish.
Or duzen and siezen.
Doctor Doctor
https://www.youtube.com/watch?v=FwNOmS78q-o
Finally somebody gets it right. A hugely underrated band.
You’re not. ?
Boo…late to the party again. Sean, hows the lockdown in the Quakertown?
I’m at work.
*shrug*
The whole shutting down liquor stores is rage inducing, but I’m very well stocked right now.
We ar elooking to go the same way up north as well. The liquior store thing will just result in my wife and I consuming the old stock in the cabinet so we can replenish with fresh stuff later. I do expect us getting out the Playboy bartender bible to figure out what to make with the more obscure stuff.
Talking to the Lowe’s delivery guy today, he said the Quakertown store was mobbed over the weekend. Crazy busy.
So much for social distancing and sheltering in place. *snicker*
Grocery shopping was very normal on Saturday and the range was busier than average on Sunday.
I spend the past weekend building a range shelter/hut with my shooting range benefactor. We built a 18′ X 6′ shelter that will have AC and heat for the winter. We have 50, 100, 150, and 200 yd steel as well as various shorter range steel targets. It’s going to be a fun summer.
The gun shop was all out of Glocks and ARs this past Saturday. All of the panic purchasers were in to buy their first noise makers.
Nice! x2
I’m not and if they pull that shit here I’ll be severely disappointed.
I was shocked how bare the liquor shelves were at Sam’s Club/Walmart, and this is in a college town with everyone on break. People were literally throwing the last cases into carts.
Plan ahead.
They at least gave us a sporting chance and warned us with just enough time to panic buy extra.
Just picked up a couple 1.75’s of vodka. And another week’s supply of Juuls.
Ya know, not one month ago, I decided to downsize my liquor collection since I’ve moved away from cocktails and more into wine in recent years… Kinda regret it now.
Oh well, I’ll swing by the liquor store on the way to work today. Just like with food, I can live on weird shit that nobody else likes.
NH’s are still open for business.
“Doctor, doctor…..glad I’m not sick!”
I have no problem using “Doctor” when talking to a medical doctor or a Phd in a professional environment. Out side of work it will be their given name or a nickname of Doc and in “what sup doc” for a medicl doctor only. My SIL and BIL are both full of themselves Phd holders. Both have a Phd in very technical fields (CompSi and Biochemistry), but they are never going to hear me refer to them in any other way than by their given name or my made up version of their names.
that’s the proper attitude
I mean, as long as you get xer pronouns correct
I usually use Dr. McDrunky or Carolina Fats as my nick names. This is usually between my wife and I, I’m not a complete a-hole.
“Hey dicknose!”
That is Dicknose, Esq. you peasant!
DOCTOR Dicknose!
In the Army (at least back in my day) almost any medical personnel were addressed as “Doc.” An E-3 Company Aidman attached to an infantry platoon was invariably called “Doc” by the 11B guys.
Yep, same for me. Doc was right up there with God in the pantheon.
+1
Million to one shot doc.
https://www.youtube.com/watch?v=IulcfUm-cUM
Yup – NOBODY is more protective of “doc” (every Navy corpsmen was called that) than the Marines I saw in Afghanistan. Of course, some of the shit those guys did…. *shivers* I guess I would be too.
In five years in the Corps, never saw a corpsman address as anything other than Doc
Yes, absolutely. Who uses titles socially regardless of degree or profession?
People who attended a cooking school?
Judges. They really get off on that.
+1 Judge Smith at my gym
Yep, that’s a good one. Judge Snails…
Someone explain to me how a curfew in New Jersey is going to affect transmission.
Coronavirus is a night owl.
Because governor Murphy is an idiot looking for any excuse to get his authoritarian on.
who knows what happens in he dark? be afraid of it
A curfew is going to increase transmission by forcing people into a smaller window of time to get their work and errands done, thereby forcing people into more contact than otherwise.
Igh. This is more like the L.A. riots than 9/11. Anyone else here remember?
+1 rooftop Koreans.
I was building the Arco training center, in La Verne, and they shut us down for a week, 30 miles from the riots, fuckers!
Am relieved to see that you’re OK, Yusef.
What happened to South Bay Glibs even before this mishegas?
Is that where the gas attendants from New Jersey and Oregon learn the secrets of the trade?
I was studying in Russia that spring. Thankfully.
Ugh, she meant to say…
For Tundra: Done shopping
There are actually a lot of funny ones at Powerline
That shit was so Boomer that I aged 20 years just by reading it.
Its so boomer i’m now at risk for the coronavirus.
Bravo!
“Sparkling Isolation” Awesome!
Two type of people in the world.
*sensible chuckle*
LOL!
Those old asian women are tougher than they look!
Developing story:
China Bans All U.S. Nationals Working for The Wall Street Journal, New York Times, Washington Post Whose Press Credentials End in 2020
https://www.wsj.com/articles/china-bans-all-u-s-nationals-working-for-the-wall-street-journal-new-york-times-washington-post-whose-press-credentials-end-in-2020-11584464690
Ha. Jokes on them. If you Ban All U.S. Nationals Working for The Wall Street Journal, New York Times, Washington Post Whose Press Credentials End in 2020 then only outlaws will have U.S. Nationals Working for The Wall Street Journal, New York Times, Washington Post Whose Press Credentials End in 2020
Fuck off China, then keep fucking off.
Given the diligence with which those organizations have carried water for the ChiComs, this seems rather ungrateful.
They didn’t carry enough water. After all that money spent on them they still fell short, so the Chicomms are cutting their loses.
Medical school admittance is tightly controlled by the AAMC guild.
Isn’t this something Dr. Groovus used to bitch about not being true? Or am I think of something else?
Another asks whether the “lack of minorities such as African Americans or Latinos/Latinas among university faculty members” is due to symbolic racism, institutional racism, hidden racism, or personal bias (the correct answer is institutional racism).
Fuck.
For example, new physical therapists are now required to obtain a doctorate in physical therapy to practice. However, the doctorate program just replaced the former master’s program without any progression.
I noticed my old PT sported his doctorate in Physical Therapy, though usually it was to poke fun at the credentialism. I think my new PT does not have a doctorate. She’s been practicing for at least 30 years. She is also much better in my opinion than my old PT.
Nice write-up!
Coronavirus freak-out update: I got some Guinness stew for take-out from the local Irish pub for lunch. It was eerie walking in there as it was completely empty and the only sound was the TV over the bar. Off in the one corner was a family waiting for some take-out food. My food was ready when I got there. One of the managers was running food in and out of the kitchen. I think the only other staff there were the kitchen guys. My total was 16 or so. I handed the manager a 20 and told her to keep it. The stew was good.
Thank you! I’m not sure what Dr. Groovus was referring to. I think we could easily double the number of medical schools in this country without any impact on the technical ability of admitted students.
We got some pizzas for lunch today from a local Italian place. It’s a gem with a deli and wood oven. I’m try and give a little extra business over the next month or two and hope they can weather this.
We have a place like that nearby. It’s awesome. They have a little market attached to the building where you can buy imported wines, olive oil, pastas, cheese, and all other kinds of Italian delicacies.
And the food was AMAZING. I had fried calamari with aioli, rigatoni with vodka sauce and chicken parmigiana, and finished off with espresso and a large cannoli.
De Blasio – New York may be under a shelter-in-place order within 48-hrs.
This is your warning notice Rhywun. Buy booze.
This is your warning everyone. They have only been a few days ahead of the rest of us.
Fair point.
Yep, I’m expecting it by Monday.
The military bases are probably going to essential personnel only in a very short time frame. That’s about 50% of our region.
NN, right?
I was planning to be out there next month. Looks like that ain’t happening.
If it does, let me know. I’ll peek out of my bunker and wave at the minimum, but more likely I’ll buy you a drink if there’s a bar still in existence.
Rumour has it that similar orders will be given throughout Canada within the next day or so.
Just did. And I’ll probably go again for more tomorrow.
“Is it just me, or is the water in this pot starting to get pretty warm?”
+ 1 ribbit
Hawt.
Nah brah — It’s awlays been like this.
https://tenor.com/view/heavy-rain-golf-caddyshack-bill-murry-heavy-stuff-wont-come-for-quite-awhile-gif-14870386
You want a title? How about…
His Excellency, President for Life, Field Marshal Al Hadji Doctor Idi Amin Dada, VC, DSO, MC, Lord of All the Beasts of the Earth and Fishes of the Seas and Conqueror of the British Empire in Africa in General and Uganda in Particular
My father always said he would settle for a good genuflection and the title Lord.
Lord of All the Beasts of the Earth and Fishes of the Seas
This is how you title. No room for half-measures.
At least he didn’t claim to be the Last King of Scotland.
Ruh-roh. Total Wine isn’t taking on-line orders.
CODE RED. CODE RED. IMPLEMENT EMERGENCY ACQUISITION PROCEDURES IMMEDIATELY.
Looks like I should stock up a bit more as well. While I am acquiring cheap wine at Food Lion I will see if there is any chicken because, for some reason they had none this past weekend.
The SJW crap in medical school is designed to:
A) Get physicians on board with socialized medicine
B) Make it easier for them to disregard the Hippocratic Oath when we inevitably start withholding medical care from wrongthinkers
Commies are very savvy in their understanding of how to dominate the population. Controlling education and healthcare gives you complete control over the population. You must parrot their ideology or… whoops! I guess you can’t use our dialysis machines anymore Mr. Deplorable. Sorry! Oh jeez Mrs. Bitterclinger, you’re no longer qualified to receive that heart medication. And don’t you even think about using the private market or going outside the country, that’s illegal and you’ll go to prison!
These are good points. I think it’s also herd mentality. Even without that endgame in mind, they can’t resist peddling the SJW crap.
I’m the only white male in my PhD program. The only one. I remember sitting around the room when my school colleagues started going on about the obstacles for women and minorities becoming students in health care fields. I looked at them like they each sprouted two heads and were speaking gibberish. Even faced with the overwhelming absurdity of such statements in their own lives, they still just can’t help themselves. It was unreal.
EU voted to close all external borders.
lol, for real? ours already too late for them, or are they doing it to protect everyone else?
Too late.
And racist, or so I am told.
Meh, it was already too late for everyone who did it. At least the smugness will be dialled down n— oh who am I kidding.
“However, the doctorate program just replaced the former master’s program without any progression. This move to doctorates is coming for the other types of therapists too”
Not exactly, it is a year longer program now. the upside is that pts can provide services without needing an M.D. to write a script.
My OT wife thinks it’s buckshot. both her needing a prescription to treat and the ‘ doctorate’ that pts get now. Outs credentialing, but it’s also the schools making an extra years worth of tuition.
Yes, you’re right. I phrased that poorly. What I meant was that the doctorate is replacing the master’s. It’s not a progression from a master’s to the doctorate. It’s just the master’s re-bundled with a little extra for that extra tuition you mentioned.
And I’m not trying to downplay PTs at all, or the work they do to get their degrees. It’s just highlighting credentialism creep and happens to be the example I know of in real life where someone with a doctorate insists on being called Dr. So and so in social situations.
I recently ran into a Doctor of Business Administration. His wife was the one who was insistent on it.
My sister is a librarian. Apparently, prior to 1971, the only qualification was being quiet and bookish. Then one of the CA schools (UC Berkeley or UCSF, IIRC) created a graduate program in Information Sciences. Now, many years of schooling are required to successfully put books on the shelves in some semblance of order and keep the homeless from looking at too much porn on the computers.
Stock market up today. bought a bit early today/late yesterday. did i get in on the floor or are we still headed way down?
I’m guessing the volatility reigns for another couple weeks, and if the panic hasn’t subsided by then, it’ll be a major drop.
Decline isn’t over. Not sure where the floor is, but Goldman is predicting S&P500 to hit 2000 before it’s over.
crazy. well i still have a lot of gas in my tank, plan to keep buying if it goes down more or stays about where it is now.
Tsar Vlad.
https://pjmedia.com/vodkapundit/reset-russian-parliament-declares-national-do-over-allows-putin-to-rule-until-2036/
Russians know what they like, and they like dictators.
Just name him Czar. It’s what he is in fact. It also appears to be what the Russian people want as long as they chose Czars who aren’t idiots, so who am I to complain.
Our mobile pet grooming business is prime for this hysteria, we offer no contact pickup and dropoff of pets and can accept digital payments. However I can only assume with SF locking down and soon NY…Vegas wont be that far behind.
If so there goes close to half our income.
Oh and a sizeable investment for the startup. Fuck all these fucking fucks
Would you come to BhC? Bella needs a bath…..
Seriously
Michigan has 58 COVID cases and Ohio has 52.
They finally beat us at something.
Today’s update says 67! In yer FACE, M state!
Good article. I’m still of the opinion that “doctor” should be used only by medical doctors, as that’s the colloquial usage of the word, but I get why the other doctors want it too since they had it first and people don’t like words getting redefined by popular usage (and I am often in that camp). It is interesting how it came about though, that “doctor” was any one educated sufficiently to be considered a master in their field, then people demanded medical professionals get this, then since most people interact with medical professionals but not educational masters the term “doctor” became associated almost entirely with medicine, then we had the explosion of university education and credentialism and now there are other doctors out and about in the wild. And to me, personally, a non-medical doctor using the title doctor will always come off as a bit pretentious, like people using the title “Senator” or “Colonel” or “Reverend” when they are no such thing (anymore).
Except for Col Sanders.
Well, I never.
I think there’s also context: if you’re calling me doctor at work I don’t think it’s pretentious. But, I strenuously object to people using the title outside of that situation.
“deer” once meant pretty much any four-legged critter
“girl” once meant pretty much any prepubescent child
“celibate” once simply meant “unmarried” and “chastity” meant, well, “chastity”
“engineer” once meant “contriver” or “inventor”. . . . now every systems analyst is an “engineer”
* gives up *
The knob-slobbering press referring to the Attorney General of The United States as a military rank angers me to no end (they kept calling that prudish dolt “General Ashcroft” through the entirety of Bush the Lesser’s administration).
deer once meant pretty much any four-legged critter
girl once meant pretty much any prepubescent child
celibate once simply meant unmarried and chastity meant, well, chastity
engineer once meant, essentially, inventor. . . . now every systems analyst is an engineer
* gives up *
the meaning of squirrel, however, has evolved.
Interesting, I did not know that about “deer” or “girl”. Language is fascinating.
I love English even though I’ve barely touched its surface in half a century.
English, as I wrote about myself earlier, is a product of the North Sea. The history of those tides is more than you can soak up in a lifetime.
I really like the place names around Leeds: some AngloSaxon, some Gaelic, some Norman . . . and the translations.
hang on: your post will post
in two minutes, apparently
We’re witnessing the redefinition of ‘squirrels’ in process.
Since it comes up from time to time, here’s a review of potential treatments for covid-19
https://sph.nus.edu.sg/wp-content/uploads/2020/03/COVID-19-Science-Report-Therapeutics-13-Mar.pdf
Where is the Three Bs treatment?
Booze, Blow & Bitchez…
See upthread for TCM.
needs more clorox
Best. Timeline.
https://www.tmz.com/2020/03/15/nevada-brothels-demand-masked-sex-during-coronavirus-scare/
I AM ZORRO!
If you’re banging hookers, you’re probably not that concerned about germs in the first place.
Now’s the Incels Chance!
Related:
https://apnews.com/62a2ea1dc6b3bf7d10b1d7305dc1a391
Won’t someone please think of the whores!
I just posted a reply and it said ‘your comment is awaiting moderation’?
Is this happening to anyone else?
I don’t recall getting cat-butted.
^(^
(*)
This virus is affecting literally everything.
The filter detected COVID-19 on your post.
Ditto
I’ve gotten that twice now.
Mind trying again C? I’m interested in your thoughts on this, especially if you see a difference in very recent med school grads versus older physicians.
It went through. Good points about maybe the SJW edge getting blunted over time.
This below got the moderator thing as well, so trying again without the quotation marks, perhaps thats it
What we’re seeing of today’s younger docs is not so much the social justice-heavy mindset, although there are plenty of those, but the prevailing difference seems to be an unwillingness to ‘work your way up’ like we older docs all did.
They all seem to expect day one out of residency to get a high-paying position that’s only day shift hours Monday-Friday with no call, no weekends, and plenty of perks and tons of vacation, etc. And many of them are actually getting it, so doc-hungry practices are giving the youngins these wonderful positions, leaving the guys in their 50s and 60s to handle the overnights, weekends and holidays.
Well, bless their hearts for being able to pull it off. But many of these same young docs, being born after the fall of the Berlin Wall, are also supporters of Medicare for All, and if that ever happens, I think they will be stunned at how precipitously their salaries drop while their working conditions deteriorate just as fast, leaving them saying but wait! I never thought this would happen to me! Yes, I’m sure you didn’t, participation-trophy-winner as a kid who is now a physician.
I was able to get it to go above and now it’s a double post, but oh well.
What we’re seeing of today’s younger docs is not so much the social justice-heavy mindset, although there are plenty of those, but the prevailing difference seems to be an unwillingness to ‘work your way up’ like we older docs all did.
They all seem to expect day one out of residency to get a high-paying position that’s only day shift hours Monday-Friday with no call, no weekends, and plenty of perks and tons of vacation, etc. And many of them are actually getting it, so doc-hungry practices are giving the youngins these wonderful positions, leaving the guys in their 50s and 60s to handle the overnights, weekends and holidays.
Well, bless their hearts for being able to pull it off. But many of these same young docs, being born after the fall of the Berlin Wall, are also supporters of Medicare for All, and if that ever happens, I think they will be stunned at how precipitously their salaries drop while their working conditions deteriorate just as fast, leaving them saying “but wait! I never thought this would happen to me!” Yes, I’m sure you didn’t, ‘participation-trophy-winner as a kid who is now a physician’.
Thanks for sharing that. Very interesting and seems like there might be similar parallels to Millennial attitudes in other fields, though with the shortage of physicians being an outsized influence.
Both dad and granddad were Drs. in private practice. Granddad was barely middle-class and my dad managed upper class..retired at 60. My dad confided in me that he never in his wildest dreams thought he would make the kind of money he made. There was a bit of resentment between the two about it.
#MeToo
so I re-posted after deleting a dozen quotations marks and it went through
#PostHocErgoPropterHoc #Winning #BadLogicTakes
It’s not Bad Logic if it works!
you should see the things I’ve read on warranty narratives
or, more to the point
you should see the warranty narratives I’ve shot down and refused to pay for
Wubonic Plague comment rationing. Happening to me too. I suppose this comment will also need moderation. But I have always been moderate, except for being a radical for individual freedom.
Reply to Tres with no links or funky formatting awaiting moderation. WTF?
It doesnt like {{{you}}}
Hmmm. Is it possible to get a confluence of [({them})]?
GT has shiksappeal !
Open wallet, remove pants and bend over.
https://finance.yahoo.com/news/upside-down-world-negative-rates-100000573.html
My brother had a professor (with a Ph.D) named Travis Doom… He’s literally Doctor Doom.
I’ll make an exception for him.
So I snuck a visit to Chicago in this last weekend, and before the restaurant closures slammed down managed to enjoy the
deep-dish pizzaunique-Chicago-variety-of-casserole at Pizzeria Uno with the son and his girlfriend. Four cheeses and pesto – it was glorious, whatever you care to call it.I got a kick out of watching our county health department presser, with the head of the combined health district stressing ‘stay 6′ away from each other’
The ASL interpreter was about 18″ from him, and the people poised behind (sheriff and 2 POS commisioners) were essentially shoulder to shoulder.
They keep telling their wives that that is 6 feet
Rules for thee, not for me.
Pursuant to the SJW infection of the MCAT, this is pretty interesting overall, but delves into a disturbing bit – the wokeness of young conservatives.
“Reform Conservatism”
HM can i get a ruling on the abuse of language here?
That chick from The Hunt has really nice cans.
Haven’t stocked up and worried about what’s on the menu for the next few weeks? if our little market is any indication, you for forget any french toast, but you might want to look up some lima bean recipes. They’re the only thing left in the dried legume/bean/grain section.
The comment about recipes was just rhetorical – please don’t think you have to provide some (looking at you, Mo).